   Introduction to the Gardasil vaccine The Gardasil vaccine has been considered to be a breakthrough vaccine for women and women's health, marketed incorrectly and somewhat ironically as "the cervical cancer vaccine", allegedly for the prevention of cervical cancer. But does it really do this? No! The Gardasil vaccine is not going to prevent cervical cancer, as it is an HPV vaccine - a vaccine against the Human Papilloma Virus (HPV), a viral infection that is mostly, but not completely, a sexually-transmitted disease. With over 100 HPV viruses in the wild, can this vaccine really prevent an HPV infection or even cervical cancer? Again, no! In 2007, the first Gardasil vaccine became available for public use, containing 4 strains of HPV - 2 which can cause genital warts, and 2 that may cause cervical cancer. Hence this version is now known as Gardasil 4. In 2018 a new Gardasil vaccine became available, with 9 strains of HPV viruses - still a long way short of the 100 possibles (WHO, 2019). The Gardasil vaccine was initially given only to girls of pre-teen or teenage years. In more recent times, teen boys are now recommended to get this vaccine too, as while they do not have a cervix, they too can carry the HPV vaccine and infect their sexual partners. This article will look at what you are not being told about this vaccine, why it is one of the most dangerous vaccines to ever come onto the market, and why you need to read this and confirm this information, BEFORE you inject your children with it... This is called "informed consent" - the right to know what you and your children are being injected with in this medical procedure, of the risks vs benefits, side effects and possible adverse outcomes of which there are many, so that you can make up your own minds as to whether you wish to submit your children to this almost untested vaccine, and the right to decline based on being given this information. Yes Gardasil is "almost untested" is actually true - it wasn't tested in a true scientific way, as explained in these referenced facts below. In this article and the following facts, I will refer to the original Gardasil vaccine as "Gardasil 4" to differentiate it from information from the new 2018 version of "Gardasil 9". The following is a summary of key points in the history, testing, and use of the Gardasil vaccines, including side effects and severe adverse reactions:
Risk factors for contracting HPV and development of cervical cancer Studies have shown that cervical cancer isn't only caused by the HPV virus. In fact, other causative factors must also occur for the development and progression of cervical cancer, especially:
Other factors which can increase the risks of HPV and cervical cancer include (Burd, 2003):
If these risk factors are identified and minimised, the risks of contracting HPV and it causing cervical cancer can be greatly reduced. All without a dangerous vaccine. Independent investigation into Gardasil 9 In 2019, an independent team of Italian scientists from a group called Corvelva, started investigations into many common vaccines and their ingredients. They reviewed the Gardasil 9 vaccine ingredients from several batches, looking at the genetics of the RNA and DNA of the pathogens and other ingredients in the vaccine. They found the following (Corvelva, 2019):
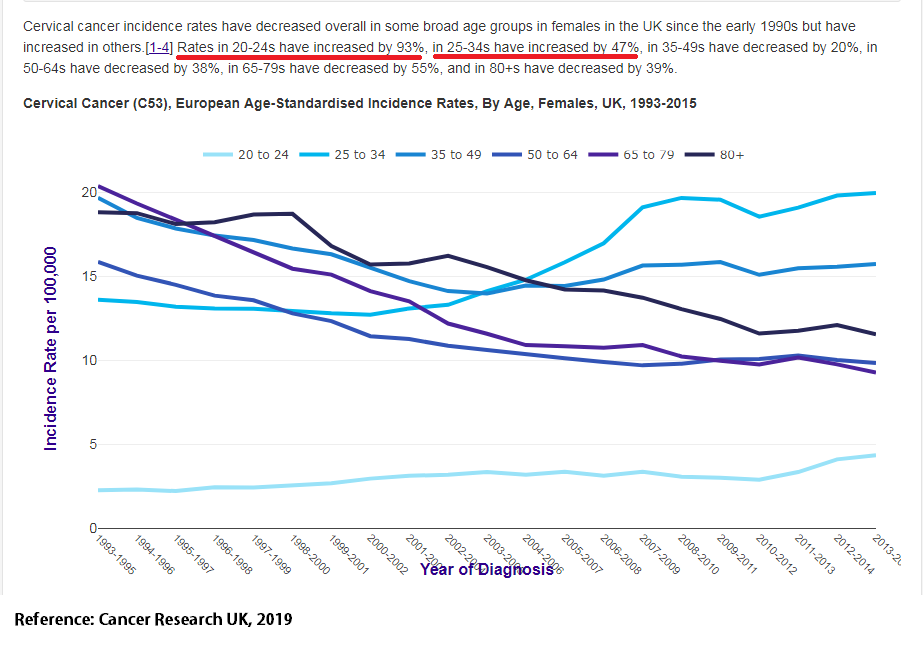
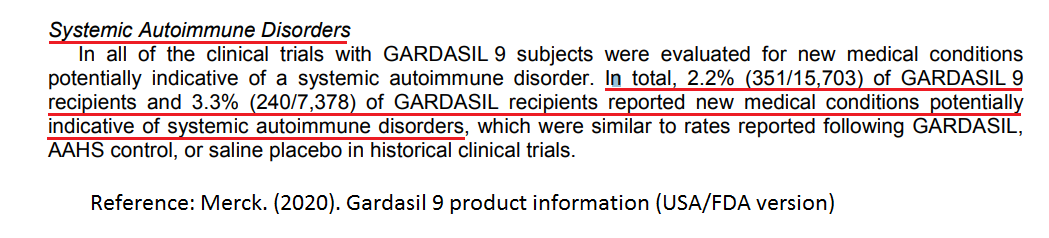
Clinical Observations In my clinical practice, I have seen many female patients who have presented with very strange symptoms that no doctor was able to find the cause of, or diagnose, or be able to treat to reduce their symptoms. My detailed questioning in my initial consultations picked up on the onset of their symptoms, which was around the start of their teen years. On intuition initially and lately from experience, I asked what may have happened at that time, or whether they had the Gardasil vaccine. In many cases, they said the symptoms appeared shortly after this vaccine. Sure this is what is known as “anecdotal evidence” but the published evidence referenced here, and from many more studies since the Gardasil vaccine became available, confirms that these side effects and adverse reactions are from the vaccine and are very real. Because doctors don't try to trace the root causes of health conditions, they don't know that Gardasil has these reactions. This can lead to the patient suffering for years to a decade or longer before being diagnosed, if at all. A very common ongoing adverse reaction I have seen in practice is a combination of chronic digestive complaints together with heart symptoms. The heart symptoms often present as a racing heart (tachycardia) which the person may or may not feel, or slow pulse (bradycardia), or arrhythmias (irregular heart beat), or having all of these - a fast heart beat becoming slow then racing again in quick succession. Heart rate testing can show a very wide range of beats, often a difference of 20+ beats per minute from low to high and low again when rested. Orthostatic testing of heart activity, of testing blood pressure and pulse when laying down, and immediately on standing, can show a steady BP but an even higher pulse rate on standing, and an overall difference in pulse of 30-40+ beats per minute. In teens who have these symptoms, many cannot tolerate any exercise, and some athletic teens have had to give up on their sports because of a sudden reduced performance after their Gardasil vaccination. Other related symptoms from the heart dysfunction include frequent fainting and dizziness, headaches, weakness and fatigue, chest pain, shortness of breath, poor thinking or low memory and concentration (NHS, 2019). Together with the irregular heart function, the same patients also have chronic digestive complaints, of pains, cramps, IBS (Irritable Bowel Syndrome), Ulcerative Colitis, hypochlorhydria (low stomach acid), chronic nausea, and other digestive complaints. The digestive system is affected together with the cardiovascular system, as both systems are controlled by nerves, or more particularly, branches of the autonomic nervous system. The dysfunction of these systems can suggest a diagnosis of Dysautonomia, or "dysfunctional autonomic nervous system". The particular dysautonomia diagnosis I have found as a direct result of the Gardasil vaccination is Postural Orthostatic Tachycardia Syndrome or POTS. In my investigations of many patients with Gardasil reactions, I have diagnosed POTS from their symptoms, history, and orthostatic testing of their blood pressure and heart rate. I have referred patients to their GP for a formal testing and diagnosis, only to be told that they don't know what POTS is or who to refer to. Luckily, POTS can be diagnosed, treated and reversed, but not with medical interventions. It can be treated with nutritional medicine, lifestyle improvements, and herbal medicines. I have also seen cases of cervical cancer being diagnosed in women who tested negative for HPV, but some had the Gardasil vaccine (which is known to cause cervical cancer). They also had hormone imbalances, and other factors like stress and nutrient deficiencies. Conclusions This document is a summary of many published studies into the Gardasil vaccine, information from the manufacturer, official government statistics, information from drug regulators, and from my own clinical experience with patients who have had many side affects, adverse reactions and chronic health conditions resulting from the Gardasil vaccine. The Gardasil vaccine was not thoroughly tested, and not tested to accepted scientific protocols before being approved for use. Testing did not include using an inert placebo in the control group, which enabled the manufacturer to claim very little difference in side effects between the vaccine and an active placebo. This is an unconscionable act which was done deliberately to hide side effects in order to gain a fast approval. It also shows a lack of thoroughness of the drug regulators to not see this deliberate ploy of deception, prior to the vaccine being approved. The Gardasil vaccine does not do what it claims to do - to reduce incidences of cervical cancer in women. In many countries, including in Australia, cervical cancer incidences have increased every year since Gardasil was introduced. And any protection from antibodies has only a short lasting effect of 4 years. After this time, there is no immunity to HPV. Gardasil has been shown in studies to actually cause cervical cancer. Gardasil simply does not work. Gardasil causes many side effects, long-term health effects, and causes many deaths. One of its key reasons for this is the use of an aluminium adjuvant, used to heighten the immune response to producing antibodies, and many recipients still do not develop antibodies to HPV. Aluminium in the body is a neurotoxin - it damages nerves of the autonomic nervous system, to cause a great many symptoms and health issues, such as heart conditions and digestive conditions. HPV alone is not the only cause of cervical cancer - an imbalance in male and female hormones and a dysfunctional immune system are also required factors for the development and progression of cervical cancer. Improve the immune system function and improve the hormone imbalance and cervical cancer can be prevented or reversed, without needing the dangerous Gardasil vaccine. All parents of teenage children must be given full informed consent of all the risks of the Gardasil vaccine, including the chronic health conditions and reactions it can cause, including death. I do not see this information being given to parents or teens. Where there is a risk with a vaccine, and there are many with Gardasil, parents and teens must be fully informed and also allowed the right to decline this medical procedure. Luckily there are other options available to reduce the risks of this infection and to also reduce the risks of cervical cancer. Schools around the country (and in other countries too) are the target for government-funded mass vaccination programs for the Gardasil vaccine. All Year 7s in Australia are rounded up and taken somewhere in the school for this shot. Often, letters or forms by concerned parents to not get this vaccine are ignored by teachers and the health department staff who simply assume that all children will get the vaccine. It is best to inform your children of the dangers to this vaccine, and keep them home on the allocated day, or to avoid it by hiding during the time it is being done. (The full article and references list is avaiable as a PDF download at the bottom of this page) References: Alleva, E., Rankin, J., & Santucci, D. (1998). Neurobehavioral Alteration in Rodents Following Developmental Exposure to Aluminum. Toxicology and Industrial Health, 14 (1-2): 209-21. doi: 10.1177/074823379801400113. Beppu, H., Minaguchi, M., Uchide, K., Kumamoto, K., Sekiguchi, M., & Yaju, Y. (2017). Lessons learnt in Japan from adverse reactions to the HPV vaccine: a medical ethics perspective. Indian Journal of Medical Ethics, 11 (2). Doi: 10.20529/IJME.2017.021 Burd, E.M. (2003). Human Papillomavirus and Cervical Cancer. Clinical Microbiology Reviews, 16 (1): 1–17. doi: 10.1128/CMR.16.1.1-17.2003 Centre of Disease Control (CDC). (2020). Fact Sheet for Public Health Personnel. Retrieved 15th June 2020 from https://www.cdc.gov/condomeffectiveness/latex.html#:~:text=Consistent%20and%20correct%20use%20of%20latex%20condoms%20reduces%20the%20risk,genital%20warts%20and%20cervical%20cancer). Corvelva. (2019). Initial results on Gardasil 9 chemical composition. Retrieved 15th January 2019 from https://www.corvelva.it/en/speciale-corvelva/vaccinegate-en/initial-results-on-gardasil-9-chemical-composition.html Hu, Y. (2018). Multiple Sclerosis Development in Two Teens After HPV Vaccination. Retrieved 15th June 2020 from https://www.neurologyadvisor.com/conference-highlights/actrims-2018/multiple-sclerosis-development-in-two-teens-after-hpv-vaccination/ Merck. (2020). Gardasil 9 product insert. Retrieved 15th June 2020 from https://www.fda.gov/media/90064/download National Health Service (NHS). (2019). Postural tachycardia syndrome (PoTS). Retrieved 15th June 2020 from https://www.nhs.uk/conditions/postural-tachycardia-syndrome/ New Scientist. (2006). First cervical cancer vaccine is approved. Retrieved 15th June 2020 from https://www.newscientist.com/article/dn9305-first-cervical-cancer-vaccine-is-approved/#:~:text=The%20first%20vaccine%20against%20cervical,month%20fast%2Dtrack%20clinical%20test. Roura, E., Travier, N., Waterboer, T., de Sanjosé, S., Bosch, F.X., Pawlita, M., Pala, V., Weiderpass, E., Margall, N. Dillner, J., Gram, I.T., Tjønneland, A., Munk, C., Palli, D., Khaw, K., Overvad, K., Clavel-Chapelon, F., Mesrine, S., Fournier, A., Fortner, R.T., Ose, J.,Steffen, A., Trichopoulou, A., Lagiou, P., Orfanos, P., Masala, G., Tumino, R., Sacerdote, C., Polidoro, S., Mattiello, A., Lund, E., Peeters, P.H., Bueno-de-Mesquita, B., Quirós, J.R., Sánchez, M-J., Navarro, C., Barricarte, A., Larrañaga, N., Ekström, J., Lindquist,D., Idahl, A., Travis, R.C., Merritt, M.A., Gunter, M.J., Rinaldi, S., Tommasino, M., Franceschi, S., Riboli, E.,& Castellsagué, X. (2016). The Influence of Hormonal Factors on the Risk of Developing Cervical Cancer and Pre-Cancer: Results from the EPIC Cohort. PLoS One, 11 (1): e0147029. doi: 10.1371/journal.pone.0147029 Sequiris. (2019). Australian Product Information – GARDASIL® 9. Retrieved 15th June 2020 from https://labeling.seqirus.com/PI/AU/Gardasil/EN/Gardasil-9-Product-Information.pdf Shaw, C.A., & Petrik, M.S. (2009). Aluminum Hydroxide Injections Lead to Motor Deficits and Motor Neuron Degeneration. Journal of Inorganic Biochemistry, 103 (11); 1555-1562. doi: 10.1016/j.jinorgbio.2009.05.019. Shaw, C.A., Li, D. & Tomljenovic, L. (2014). Are There Negative CNS Impacts of Aluminum Adjuvants Used in Vaccines and Immunotherapy? Immunotherapy, 6 (10):1055-71. doi: 10.2217/imt.14.81. Vadalà, M., Poddighe, D., Laurino, C., & Palmieri, B. (2017). Vaccination and autoimmune diseases: is prevention of adverse health effects on the horizon? European Association for Predictive, Preventive and Personalised Medicine (EPMA), 8:295–311. Doi:10.1007/s13167-017-0101-y WebMD. (2020). HPV, Cervical Cancer Vaccine: 15 Facts. Retrieved 15th June 2020 from https://www.webmd.com/vaccines/features/hpv-cervical-cancer-vaccine-15-facts#2 World Health Organisation (WHO). (2019). Human papillomavirus (HPV) and cervical cancer. Retrieved 15th June 2020 from https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer#:~:text=There%20are%20more%20than%20100,the%20onset%20of%20sexual%20activity. Download, save and share this article and references, or keep for your info!
0 Comments
|
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
February 2023
Categories
All
|
||
 RSS Feed
RSS Feed